
Subacromial 'impingement'. Are we closing in on removing this term?
Article review of Hunter et al., (2021)

Paper title and link to paper:
Acromiohumeral distance and supraspinatus tendon thickness in people with shoulder impingement syndrome compared to asymptomatic age and gender-matched participants: a case control study (Hunter et al., 2021)
Overview of the paper:
The idea that there is a mechanical compression from the acromion on the supraspinatus tendon causing pathology as a model for shoulder impingement has been around for some time (Codman,et al., 1934; Neer et al., 1974).
Treatments targeting removal of this suspected compression from bony or soft tissue sources, such as a sub-acromial decompression (SAD), have shown to be comparative to a placebo operation (Beard et al., 2018). This leaves us questioning why people seem to benefit from surgical management if surgical removal of this supposed biological compression is not the holy grail.
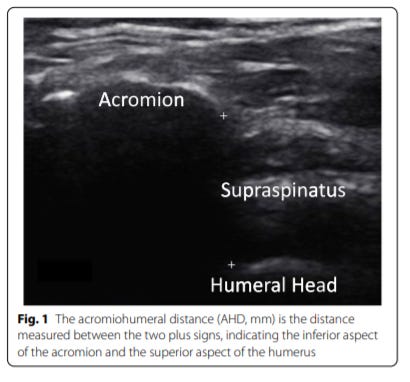
The paper we are going through this week is by Hunter et al., (2021) who used ultrasound to evaluate the acromiohumeral distance (AHD) and supraspinatus tendon thickness (STT) in people with and without rotator cuff related shoulder pain (RCRSP).
The authors first talked about previous studies who have looked into this area. They reported two studies who found a smaller AHD in those with RCRSP than in controls and three other studies who found no difference in AHD between those with or without RCRSP. The findings of these studies have been questioned by the authors who suggested that they all have some level of poor methodological quality such as using non-expert sonographers.
The current study by Hunter et al., (2021) looked at the AHD (figure 1) and STT (figure 2) in 39 individuals with RCRSP. They were compared them to 39 matched controls without RCRSP.

The authors’ found that those with RCRSP had significantly greater AHD and STT. Both reached the minimal detectable change (MCD).
Although the rest of the blog will not focus on the STT, I must note that this is a significant finding and something I am sure to pick back up on in a future blog post.
The finding that AHD was significantly greater in the RCRSP group completely opposes the impingement compression model and further questions its validity.
Being as skeptical as I am, we do have to consider a few things from this study.
The authors’ noted multiple limitations which they documented in the discussion. One of those was that in the RCRSP group, they had a significantly greater BMI which was a significant covariate for both the AHD and STT results. Was this due to poor matching in the control group or are those who have RCRSP more likely to have a higher BMI?
One further limitation that I ponder was their inclusion criteria to diagnose RCRSP. They enrolled a patient as having RCRSP onto the study if they met three criteria: (1) Shoulder pain for >3 months, (2) having a minimum of three positive tests out of Neer test, Hawkins-Kenedy test, painful arc test and the external rotation resistance test, and (3) confirmed as having RCRSP by a radiologist using USS. I question this inclusion criteria for a couple of reasons:
If someone has less than 3 months of shoulder pain, why can they not be diagnosed as having RCRSP? Are we not excluding a large proportion of patients who would likely have RCRSP and get better within 12 weeks?
Is this cluster of tests ‘the best cluster’ to diagnose RCRSP? Furthering that, do we even need to use a cluster to diagnose RCRSP?
Can we really confirm someone has RCRSP using USS as we know changes on a scan are common in those without pain (see my previous blog post which goes into a bit more detail on this)
I think I am overly critiquing the method here but you can get the gist of what I am trying to put across especially when there is no ‘gold standard’ for diagnosing RCRSP.
Now, back to the findings of this paper that AHD was greater in those with RCRSP.
Can we now finally decompress the term impingement and move on to a term which that is less nocebic to the patient and actually empowers the patient to make meaningful treatment decisions to manage their shoulder pain?
I personally use the term RCRSP, based on expert consensus. Whether that is the right term to use I am still not fully certain but one thing I am getting more and more confident about is not using the term ‘impingement’.
I think we do have a long way to go in distancing the term of impingement away from shoulder injuries and shoulder pathology. Just a quick google search of the word impingement and it makes me think we have a long way to go…

Key take away points:
The theoretical, biological and psychosocial implications of using the term ‘impingement’ within the context of a shoulder diagnosis is weakening
Although this study concludes that a raised AHD is associated with RCRSP, prior studies within this area have had mixed findings
This blog was created to consolidate my learning. Feel free to subscribe. If you have any comments, further reading or suggestions on this topic please get in touch with me on here or on my Twitter. I am always learning and any discussions are thoroughly welcomed.
Cheers,
Adrian