
ULTRA guidelines for reverse total shoulder replacement
Article review of Bardsley et al., (2022)

Paper title and link to paper:
Physiotherapy treatment for reverse total shoulder arthroplasty: Results of a patient-centred rehabilitation guideline using functional and patient-reported outcome measures (Bardsley et al., 2022)
Overview of the paper:
Reverse total shoulder replacement (RTSR) is increasingly becoming a more common surgery. In 2013, 35% of all primary shoulder procedures in the UK were RTSR followed by total shoulder arthroplasty and hemi-arthroplasty of 33% and 31% respectively (National Joint Registry). In 2021, RTSR now represented 68% of all primary shoulder procedures (National Joint Registry). This rapid rise may be due to a range of patient (e.g. aging population and complex presentations) and professional (e.g. more surgeons trained in this type of surgery) reasons (Best et al., 2021). With this in mind, we need to keep up to date with rehabilitation guidelines following this type of surgery and the changes in precautions we need to be aware of*.
Bardsley et al., (2022) just released a paper in Shoulder and Elbow on rehabilitation following RTSR. The study was looking at the outcome of patients who followed their rehabilitation guidelines. They termed this programme the ULTRA guidelines and are based on best current knowledge. The guidelines in the appendix are as follows:
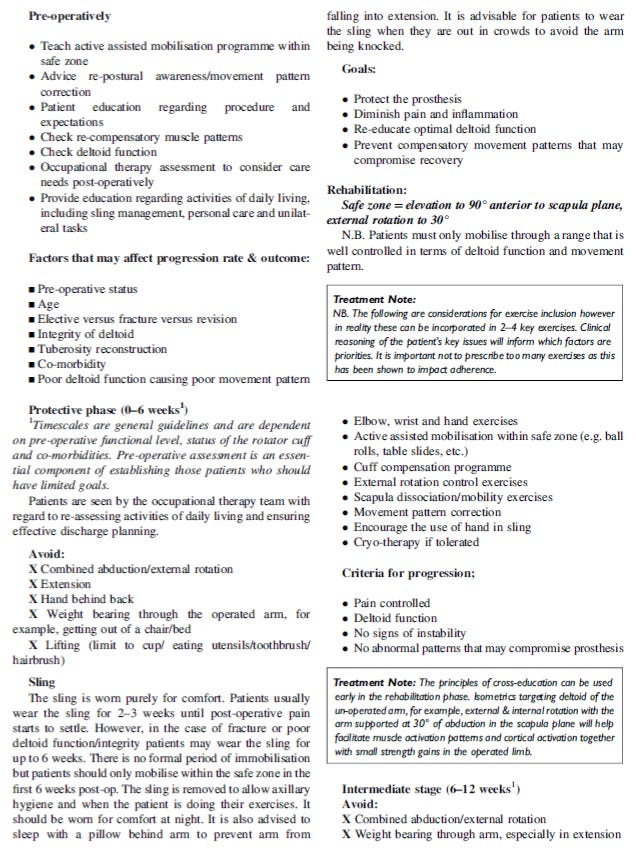
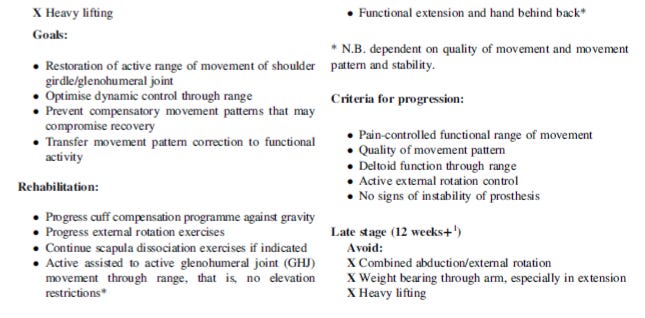
The full details of their results, including range of movement, pain levels, and patient reported outcome measures, of their patients who followed these guidelines of are found in their paper. What I am most interested in is the precautions and late stage (>12 weeks+) rehabilitation. Late stage precautions differ to a total shoulder arthroplasty where guidelines only suggest avoiding large loads through the upper limb (Blacknall and Bidwai, 2020; Kennedy et al., 2020).
For RTSR, Bardsley et al., (2022) suggests to avoid combined abduction/external rotation, no weight bearing through the arm (especially in extension) and heavy lifting. There seems to be a higher risk of a shoulder dislocation than in conventional total shoulder arthroplasty (Barco et al., 2016). Although the true mechanism is debated (Barco et al., 2016), a reverse is suggested to more likely dislocate in an extended position with adduction or internal rotation (Boudreau et al., 2007). This means simple activities such as tucking in your shirt, toileting with that arm or even pushing away to stand up from a chair may be riskier.
What is ‘heavy lifting’? I was asked this question recently by a patient and I didn’t have a good answer (and was open with them about this). Consensus on how heavy is heavy in RTSR is debated. Bardsley et al., (2022) sourced the National Joint Registry report (2022) as a supporting reference for the late stage guidelines although I cannot seem to find any details of this information in the source. Boudreau et al., (2007) suggests a maximum load of 4.5kg to 6.8kg although no note of other important variables to consider (e.g. short vs. long lever or above vs. below shoulder height). As much as I want to find a more rigid set of guidelines, it will probably be more about common sense when taking the patient individual characteristics in front of you into consideration.
As always, if anyone has any comments, further reading or suggestions on this topic please feel free to fire them at me on here or on my Twitter. I am always learning and any discrepancies on what I have written is thoroughly encouraged.
*Just to add that it is important to remember to check local policy/procedures and op notes as this will over rule the above. For example, here at Burwood Hospital, sling immobilisation is 6 weeks.