


Subscapularis. How important is it? How does it relate to cuff tear arthropathy?
Article review Furuhata et al., (2023)

This blog was meant to be focused on a new paper on progressive shoulder exercises for glenohumeral osteoarthritis and rotator cuff tear arthropathy (Larsen et al., 2022) but I slightly went off track…
Before I blog about this paper, I thought I would introduce cuff tear arthropathy and go into some depth around the subscapularis muscle which seems to be an important playmaker in shoulder health.
What is cuff tear arthropathy?
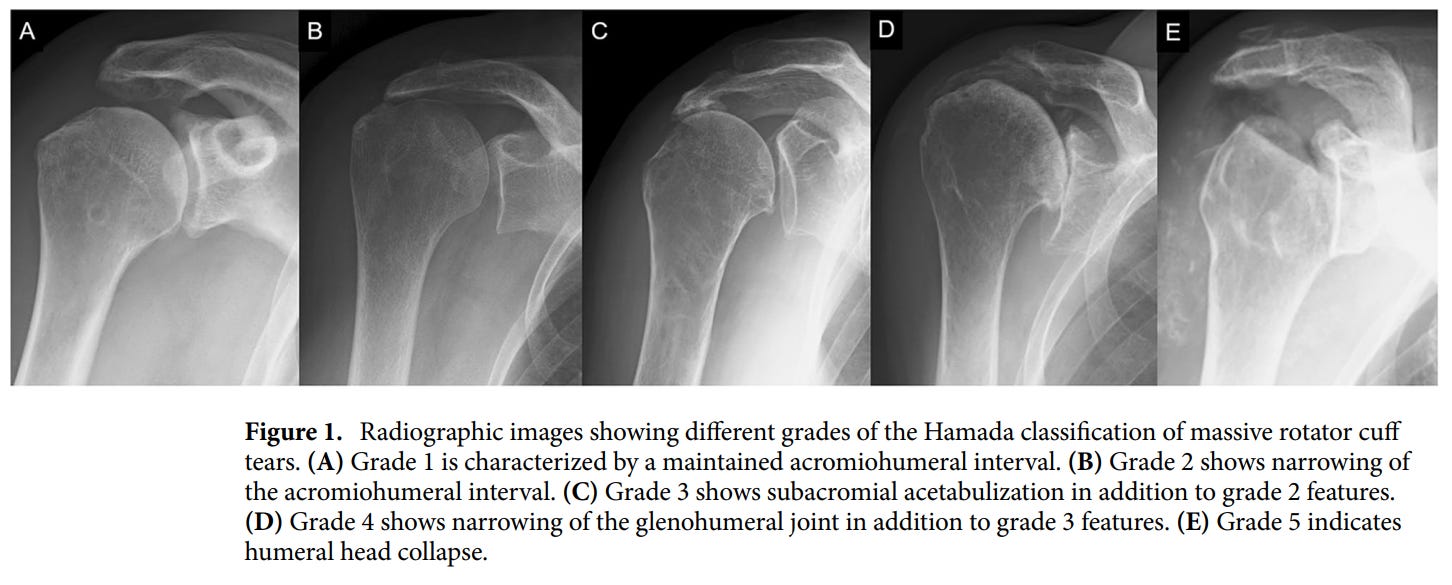
Cuff tear arthropathy (CTA) is a term used to describe the development of muscular and bony changes including acetabularization and femoralization. In the shoulder, acetabularization describes the pseudoarticulation, or the creation of a ‘false joint’, of the humerus with the undersurface of the acromion whereas femoralization describes the rounding of the humeral head.
The Hamada classification can be used to classify massive rotator cuff tears and CTA. The Hamada classification uses a grading system of 1 to 5, with the higher grades representing more changes on plain imaging. This is shown in the images below.
A closer look at the subscapularis
Subscapularis tears in particular are associated with higher grades of the Hamada classification (Furuhata et al., 2023; Hasegawa et al., 2022).
In multivariate analysis, Furuhata et al. (2022) found that superior subscapularis tears (OR = 3.23) and long head of biceps ruptures (OR = 6.31) are risk factors for narrowing of the glenohumeral joint (grade 4). They also found superior subscapularis tears (OR = 15.81), female sex (OR = 10.3), and fatty infiltration into the inferior subscapularis (OR = 5.57) to be risk factors for humeral head collapse (grade 5).
Without going too far down into another rabbit hole, something to add from this study was that Furuhata et al., (2022) split their analysis of the subscapularis into the superior subscapularis (upper 2/3) and the inferior subscapularis (lower 1/3). The authors suggests that parts of the subscapularis have slightly different functions with the inferior subscapularis having a muscular insertion whereas the superior subscapularis has a tendon insertion (Cleeman et al., 2003). These two parts of the muscle also have different innervation. The inferior portion is innervated by the lower subscapular nerve whereas the superior portion is innervated by the upper subscapular nerve (Kadaba et al., 1992).

What about functional loss with subscapularis?
It has been suggested that the subscapularis is stronger than the three posterior cuff muscles combined (Keating et al., 1993). A study by Collin et al., (2014) also highlights the significant loss of function when the whole of the subscapularis is involved. They classified their patients into the following five types.
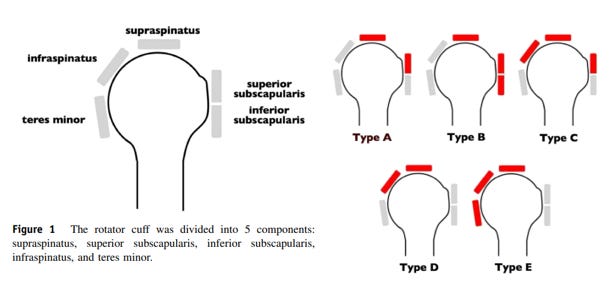
When looking at a patients range of movement, shown in the graphs below, you can see that injury to the whole of the subscapularis (type B - green bar) severely hampers flexion range of movement. External rotation seems to be relatively preserved.
The paper also found that 80% of patients with a type B cuff tear pattern had pseudoparalysis. For clarity, as definitions can vary, the authors defined pseudoparalysis as an inability to actively flex to 90 degrees with a full passive range of movement.

One thing that this study does not address, unlike the Furuhata et al., (2022) study, is looking at inferior vs. superior subscapularis involvement. All this study can tell us is that injury to the whole of subscapularis leads to poor flexion function as there was not a category of muscle tear which just involved the inferior subscapularis. It must be noted that although this study does makes a strong case for poor function with subscapularis involvement, other studies replicating this design have had variable results (Araya-Quintanilla et al., 2021; Agout, et al., 2018; Yoon et al., 2019).
What can we take away from this research?
I think the key take away points from the research on massive rotator cuff tears and CTA is the important role subscapularis plays in shoulder health and function. This biological factor can be taken into consideration as part of a bigger picture of a patient’s unique and individual presentation of shoulder pain (Lewis, 2022). Alongside psychosocial factors (Chester et al., 2018), this will help to inform decision making on treatment options from conservative (Ó Conaire et al., 2023) to surgical management (Ghasemi et al., 2023).
As always, if anyone has any comments, further reading or suggestions on this topic please feel free to fire them at me on here or on my Twitter. I am always learning and any discrepancies on what I have written is thoroughly encouraged.