

Pain drawings in those with a frozen shoulder
Pain drawings in those with a frozen shoulder
Article review of Balasch-Bernat et al., (2022)

Paper title and link to paper:
The spatial extent of pain is associated with pain intensity, catastrophizing and some measures of central sensitization in people with frozen shoulder (Balasch-Bernat et al., 2022).
Overview of the paper:
Following from last weeks blog where we talked about stiff shoulders being particularly debilitative and painful (White et al., 2022), I thought I would focus this week on another a paper on frozen shoulders by Balasch-Bernat et al., (2022).
This paper was a cross-sectional observational study (data observed at one particular time) looking at 48 people with a diagnosis of a frozen shoulder. The patients were asked about some basic demographic and pain data along with a whole range of self-administered questionnaires. They also filled out a pain drawing and underwent quantitative sensory testing (such as looking at pressure pain thresholds).
We will jump to the findings of the study then work backwards by looking at the methods. The main reported findings, noted in the abstract, were twofold:
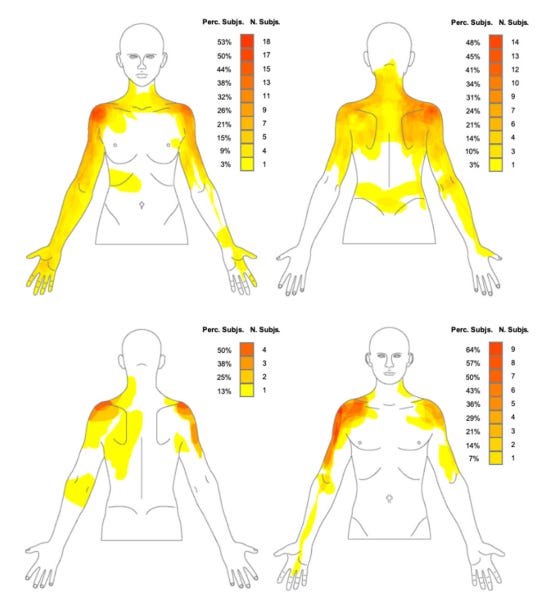
“The anterolateral region of the shoulder pain was the most common painful area in people with frozen shoulder” pp. 1
“Women with frozen shoulder presented more extended areas of pain; and a more widespread distribution of pain was correlated with higher levels of pain, pain catastrophizing and pain sensitization” pp. 1
The visual representation of the female (top) and male (bottom) pain drawings are shown below. Although the anterolateral region on the shoulder was the most common location of symptoms, you can visually see the broad location of symptoms experienced by a patient.
Now, before taking these results at face value, we need to have a look at the methods so that we can be aware of some of the limitations with the study when applying these to our practice.
Sex differences of symptoms
As noted above, a major finding was that women had more widespread pain than males in the pain drawings. When looking at the results section, the only analysis on the pain drawings with regards to male and female analysis is the following sentence:
“Women presented a more widespread distribution of pain, including the whole upper limb, compared to men”
So, a difference was found. Subjectively, you can view the pain drawings of the males and females and see there was a difference. The real question is, how large of a difference was this? Was this difference statistically significant? What were the confidence intervals? Did the confidence intervals overlap? The authors claim there to be a correlation between females pain drawings and other variables, such as higher levels of pain and pain sensitisation, yet no statistical analysis was done to compare male and female sex. The importance of this finding is thus undermined by not having this statistical analysis.
As noted in the papers discussion, the finding of women having more widespread pain was at contrast to other research on shoulder pain problems where there has been found to be no difference between sexes (Bayam et al., 2011; Gumina et al., 2014). This questions if we can really be confident with this finding.
Validity of presentation to the whole frozen shoulder population
The study inclusion criteria was a patient being diagnosed with a primary frozen shoulder (idiopathic in nature). Exclusion to the study included those with a secondary frozen shoulder. Although they did not explicitly state it, I think they also considered systemic secondary frozen shoulders as part of this exclusion.
Why do I want to make a point of this? We need to be aware that these findings may only be valid for those with a primary frozen shoulder and not of the whole population of patients suffering with frozen shoulder (Zuckerman and Rokito et al., 2011).
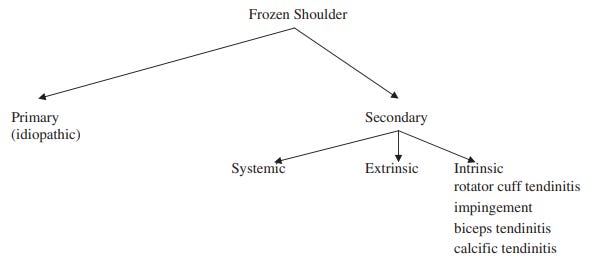
It would have been interesting to see if there are any similarities or differences in presentation in those with secondary, in particular, systemic secondary, frozen shoulders. The systemic secondary frozen shoulder group includes patients suffering from frozen shoulders with the presence of diabetes (Lowe et al., 2019). Diabetes is fairly relevant in a frozen shoulder population considering it is estimated that 30% of patients with a frozen shoulder have diabetes (Zreik et al., 2016). There is also evidence to suggest that those with a frozen shoulder who also have diabetes suffer symptoms for longer (Hand et al., 2008), are more resistance to treatment (Makki et al., 2020), and have worse outcomes (Dyer et al., 2021). Furthering this, and particularly relevant to this study, patients with diabetes have been found to have changes in nerve function and pain thresholds, even in those without symptoms of neuropathy! (Sierra-Silvestre et al., 2020). I wonder how this would manifest in a pain drawing?
What have I taken forward from this study? I feel this is an important addition to the body of literature in highlighting the diverse pain locations felt by those with frozen shoulder. I don’t think we can be confident with the findings of the distribution of pain between sexes but this is an area where further research is likely needed.
As always, if anyone has any comments, further reading or suggestions on this topic please feel free to fire them at me on here or on my Twitter. I am always learning and any discrepancies on what I have written is thoroughly encouraged.