


High vs. low load strengthening for patients with hypermobile shoulders
Article review of Liaghat et al., (2022)

Paper title and link to paper:
Short-term effectiveness of high-load compared with low-load strengthening exercise on self-reported function in patients with hypermobile shoulders: a randomised controlled trial (Liaghat et al., 2022)
Overview of the paper:
This week we are looking at a study which was recently published in the British Journal of Sports Medicine (BJSM) by Liaghat et al., (2022). The study wanted to compare two different exercise approaches, one ‘high load’ and one ‘low load’, for patients with hypermobility spectrum disorder (HSD).
One of the rationales for this study was that in Denmark, current guidelines recommended against high-load strengthening for people with HSD due to uncertainty of treatment effectiveness and safety. These guidelines were sourced in the paper as the Danish Rheumatism Association guidelines in 2015 although I have not been able to confirm this as the link provided in the paper is broken.
Methods
Participants entering the study had to have chronic (>3 months) shoulder pain and/or instability symptoms with the presence of generalised joint hypermobility (GJH). GJH was determined using the Beighton score (≥4 or ≥5 in women under 50). Patients were also included with a one point lower Beighton score if they had a positive (score of ≥2) in the 5-part questionnaire (5PQ) as shown below (Juul-Kristensen et al., 2017)

The participants were randomised into was either a “HEAVY” or “LIGHT” group which were published in a previous study protocol paper (Liaghat et al., 2020).
The LIGHT group was considered to mimic standard care. The manual of this protocol can be found in this link. This included:
Supervised initial appointment
Home programme three times a week
Supervised session at week five and week eleven when new exercises were started
Four phases of progressive exercises: (Phase 1) Postural correction, (Phase 2) static, (Phase 3) static + dynamic, and (Phase 4) dynamic. Examples of exercises used are shown below
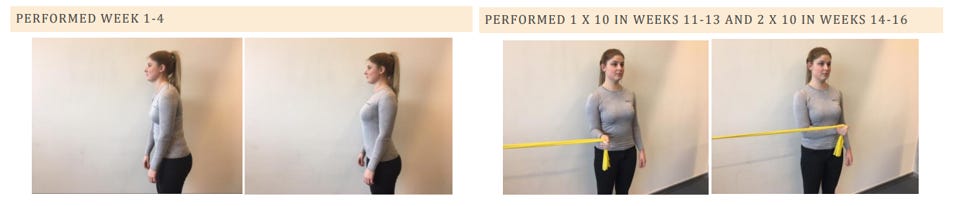

The HEAVY group was the experimental group. The manual of this protocol can be found in this link. This included:
Two supervised sessions a week
Home programme once a week
The same five exercises were used throughout the trial period with a five minute warm up. Examples of exercises used are shown below

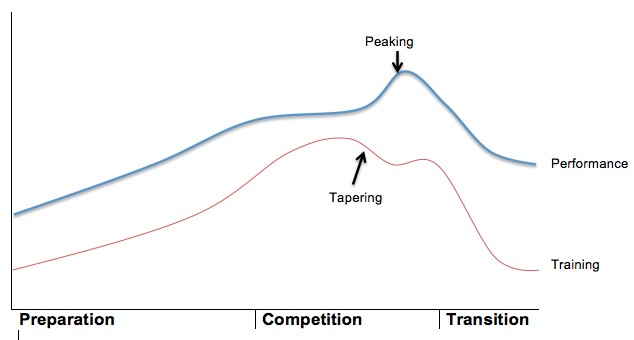
The intensity of these exercises for this protocol were calculated based on a 5-RM test (Brzycki, 1993) and modified throughout the trial period as shown in the table below. A tapering period was used in the final week prior to testing.

{kind=link}
{kind=link}

The primary outcome measure was the Western Ontario Shoulder Instability Index (WOSI). The WOSI is marked out of 2100 points with a higher score representing a greater disability. The minimally clinically important difference (MCID) used in the study was 218.4 to 294 points as per previous published data (Kirkley et al., 2005; van der Linde et al., 2017). The study was powered with this outcome measure and MCID in mind. Further outcome data taken included a range of patient reported measures (e.g. TSK-11) and objective testing (e.g. isometric dynanometer testing)
Results
Intention to treat (ITT) analysis of the primary outcome measure (WOSI) favoured the HEAVY group with a lower score of 174.5 points (95% CI 341 to 7.7). This did not reach the MCID. For those that completed the prescribed protocol (per-protocol analysis), the WOSI score again favoured the HEAVY group which this time did reach the MCID with a lower score of 250.7 points (95% CI 323.4 to 178).
The authors also looked at the proportion of patients who reached the MCID along with numbers needed to treat (NNT). In the ITT analysis, 68% and 54% of the HEAVY group and LIGHT group reached the MCID respectively . NNT was 7 in favour of the HEAVY group. In the per-protocol analysis, 85% and 55% of the HEAVY group and the LIGHT group reached the MCID respectively. The NNT was 3 in favour of the HEAVY group.
As per the secondary outcomes, the author reported generally improved findings in the HEAVY group although the majority were non-significant with large confidence intervals. Although we could delve further into the results of these outcomes, we need to remember that this study was only powered for the primary outcome measure, the WOSI. Interpretation of these results must be taken with caution. This point is discussed in a paper by Jakobsen et al., (2019) in the BMJ who suggests power estimations of non-primary (secondary) outcomes may help to bridge this gap. This will help to make results more interpretable whilst minimising type 1 and type 2 errors.
Going back to the primary outcomes, it seems that following a programme similar to the HEAVY group seems to be beneficial and something worth involving in your rehabilitation plan.
There are some points we should consider when interpreting the findings of this study. Are the changes really due to differing loads? The HEAVY group programme quantified load using 5RM calculations (Brzycki, 1993) but no such quantification of load was done in the LIGHT group. If we accept that the load was higher in the HEAVY group, we also have to question how much impact the extra supervision received in the HEAVY protocol had on the results. From these points, I consider this study to be looking at a supervised high load resistance training programme against an unsupervised low load exercise programme, rather than just high vs. low load.
One final point to make was on adverse events. This was one of the studies rationales as the guidelines by the Danish Rheumatism Association questioned the safety of heavy loading. A dislocation was classified as a minor adverse event. No patients in the LIGHT group suffered a dislocation. One patient in the HEAVY group suffered a dislocation. I was surprised to see that this was not mentioned or discussed in the discussion as for me a dislocation is probably a more important adverse event than say muscle soreness.
As always, if anyone has any comments, further reading or suggestions on this topic please feel free to fire them at me on here or on my Twitter. I am always learning and any discrepancies on what I have written is thoroughly encouraged.