

The influence of smoking on shoulder arthroplasty
The influence of smoking on shoulder arthroplasty
Article review of Kamma et al., (2022)

Paper title and link to paper:
Smoking cessation prior to total shoulder arthroplasty: A systematic review of outcomes and complications (Kamma et al., 2022)
Overview of the paper:
A tweet above by Chris Littlewood made me think back to an early chapter in Jeremy Lewis and Fernández-de-las-Peñas shoulder book on the broader influences of lifestyle factors affecting the shoulder. In this chapter, they discussed lifestyle-related metabolic disorders including diabetes and hypertension and how factors such as smoking, diet and sleep play an important role in the health and function of the shoulder.
This then leads me to a systematic review just released in Shoulder and Elbow looking at smoking and the influence on shoulder arthroplasty. The review by Kamma et al., (2022) attempted to look at evidence from randomised controlled trials (RCT) to case series. Only one cohort study (Schwartz et al., 2020) met the inclusion criteria with no RCTs. The rest of the review was made up of case-control studies and case series. As this represents the lowest levels of evidence included in the review, we have to be mindful of the potential bias in these studies.
If you wish to skip to the findings, these two sentences in the discussion sum up the review:
“This review demonstrates that smoking is significantly associated with poor clinical outcomes following shoulder arthroplasty. Current literature shows that smoking is associated with numerous postoperative complications, increased opioid use, and worse shoulder function improvement scores”
The authors (Kamma et al., 2022) make a suggestion that prior to shoulder arthroplasty:
“A period of four weeks or more of preoperative smoking cessation is recommended”
To start with, we will first look at the only cohort study (Schwartz et al., 2020) included in the review. The systematic review also suggested another paper (Hatta et al., 2017) was a cohort study but the methods in the original paper suggested it was a case-control study.
Schwartz et al., (2020)
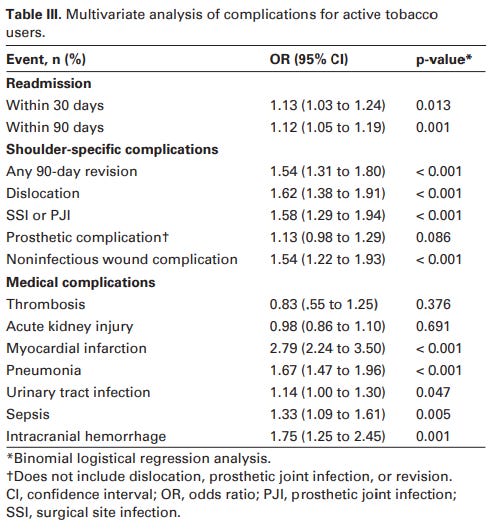
Schwartz et al., (2020) reviewed a national (USA) database of patients who had undergone total and reverse shoulder arthroplasty. While this achieved a large sample of over 200,000 patients, we have to be mindful of how this data was collected from multiple individuals and institutions. The study found smokers were at a greater risk of suffering from pneumonia, sepsis and myocardial infarction post-operatively. Smokers also had a statistically significantly higher readmission rates at 30 and 90 days compared to non-smokers. Revision rates at 90 days, wound complications, and instability of the prosthesis were also significantly higher in smokers. Odds ratios (OR) of these findings are shown below. Apart from myocardial infarction as a complication, the OR were fairly close to 1 (which would suggest no association). Although close to one, one thing to note is that in the majority of these findings, the 95% confidence intervals did not overlap 1. This gives us slightly more confidence that this may represent an association.
So, the finding from this study in the review strengthens the position of worse outcomes in smokers.
What about former smokers?
Included in the review was a study by Wells et al., (2018) which helps to answer this question. They looked at current smokers, non-smokers and former smokers. They found that:
“Former tobacco users were found to have a postoperative course similar to that of nonusers, suggesting that discontinuation of tobacco use can improve a patient's episode of care performance after TSA (total shoulder arthroplasty)”
A similar finding was also observed by Walters et al., (2020) in patients with a reverse shoulder replacement. Quitting does seem to be beneficial. Now what about time frames?
How long is long enough?
Although the authors (Kamma et al., 2022) in the abstract suggested 4 weeks or more of smoking cessation as a time frame, they admitted in the discussion that there is limited data on what the optimal time frame is. If smoking cessation is too difficult for the patient, would even reducing intake still have positive influences on shoulder arthroplasty outcomes? Potentially (Begh, et al., 2015).
This brings me to my final thought on this topic. If a patient has elective shoulder surgery, should there be a bigger drive in stopping (or reducing) smoking pre-operatively? I align this to practice here at Burwood Hospital in New Zealand where obese patients are required to hit a certain mass before they have hip and knee replacement surgery. Patients are supported by a dietitian and a physiotherapist with the overall aims (although this may be contentious) of improving surgical outcomes. Could this be replicated for shoulder surgery with the right support and guidance?
As always, if anyone has any comments, further reading or suggestions on this topic please feel free to fire them at me on here or on my Twitter. I am always learning and any discrepancies on what I have written is thoroughly encouraged.